Cms 1763 Form
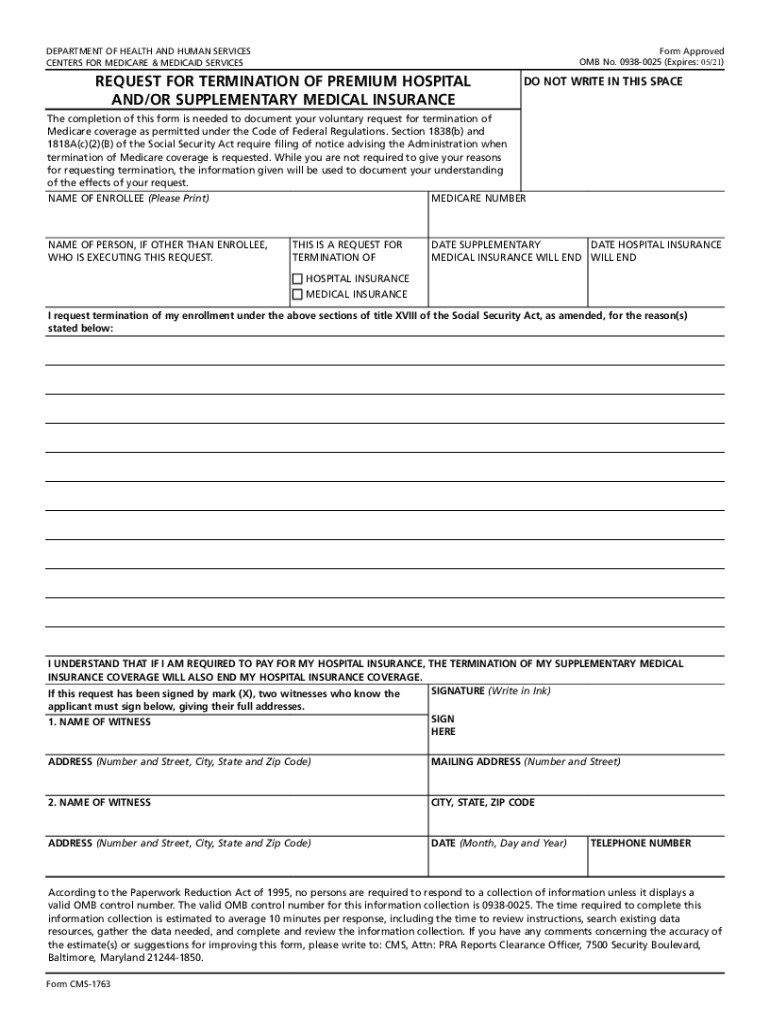
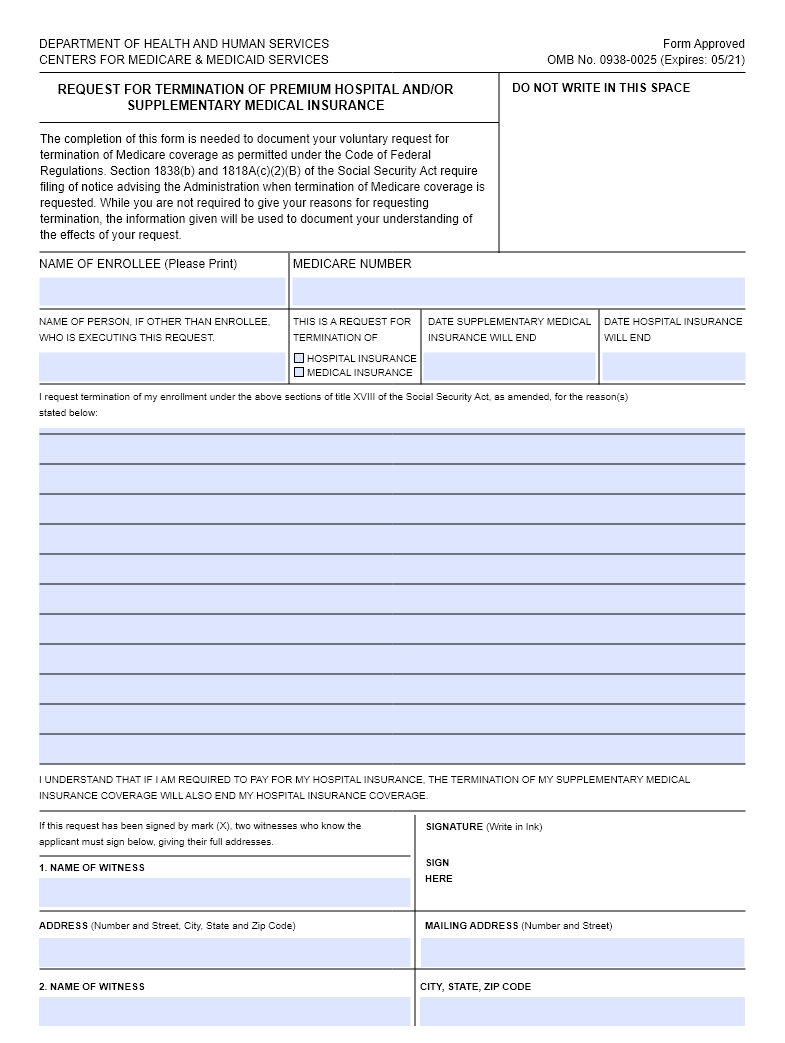
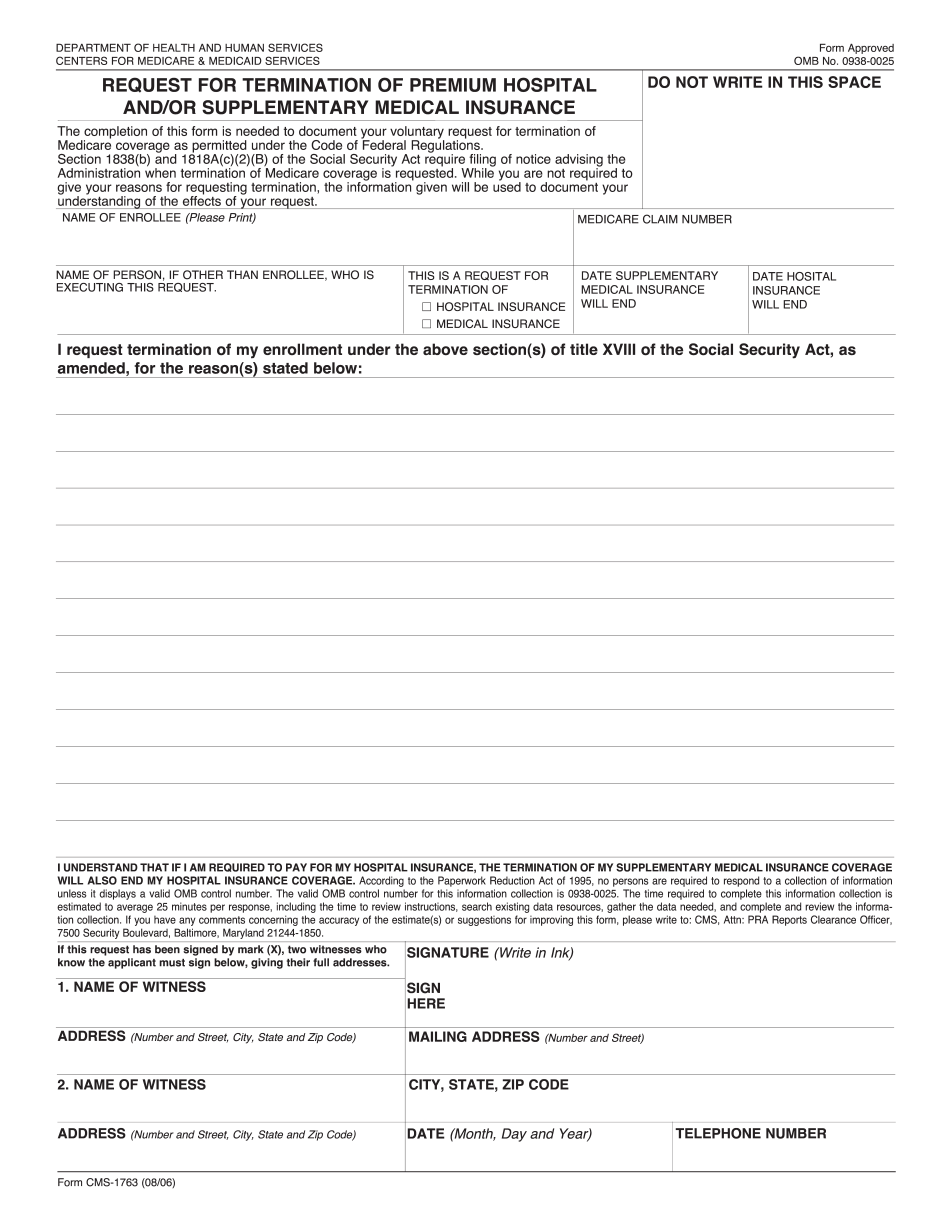
Cms 1763 Form - • if you have premium part a or part b, but wish to no longer be enrolled. People with medicare premium part a or b who would like to terminate their hospital or medical insurance coverage. Request for termination of premium hospital insurance of supplementary medical insurance. Back to cms forms list; You may also use the search feature to more quickly locate information for a specific form. You can cancel part a only if you pay a premium for it. Cms 1763 dynamic list information. The completion of this form is needed to document your voluntary request for termination of medicare coverage as permitted under the code of federal regulations. When do you use this application? The following provides access and/or information for many cms forms.
Cms 1763 dynamic list information. The completion of this form is needed to document your voluntary request for termination of medicare coverage as permitted under the code of federal regulations. Back to cms forms list; You can cancel part a only if you pay a premium for it. • if you have premium part a or part b, but wish to no longer be enrolled. Request for termination of premium hospital insurance of supplementary medical insurance. People with medicare premium part a or b who would like to terminate their hospital or medical insurance coverage. When do you use this application? You may also use the search feature to more quickly locate information for a specific form. The following provides access and/or information for many cms forms.
The following provides access and/or information for many cms forms. Cms 1763 dynamic list information. When do you use this application? You may also use the search feature to more quickly locate information for a specific form. You can cancel part a only if you pay a premium for it. People with medicare premium part a or b who would like to terminate their hospital or medical insurance coverage. Back to cms forms list; The completion of this form is needed to document your voluntary request for termination of medicare coverage as permitted under the code of federal regulations. • if you have premium part a or part b, but wish to no longer be enrolled. Request for termination of premium hospital insurance of supplementary medical insurance.

Free Printable Cms 1500 Claim Form Riset
You can cancel part a only if you pay a premium for it. When do you use this application? The following provides access and/or information for many cms forms. Request for termination of premium hospital insurance of supplementary medical insurance. Back to cms forms list;
CMS1763 20172022 Fill and Sign Printable Template Online US Legal
People with medicare premium part a or b who would like to terminate their hospital or medical insurance coverage. The completion of this form is needed to document your voluntary request for termination of medicare coverage as permitted under the code of federal regulations. The following provides access and/or information for many cms forms. Cms 1763 dynamic list information. Request.
Printable Form Cms 1763
Request for termination of premium hospital insurance of supplementary medical insurance. • if you have premium part a or part b, but wish to no longer be enrolled. Back to cms forms list; The following provides access and/or information for many cms forms. You may also use the search feature to more quickly locate information for a specific form.
Cms 1763 Printable Form
People with medicare premium part a or b who would like to terminate their hospital or medical insurance coverage. Back to cms forms list; Cms 1763 dynamic list information. Request for termination of premium hospital insurance of supplementary medical insurance. You may also use the search feature to more quickly locate information for a specific form.

Cms 1763 Printable Form
The following provides access and/or information for many cms forms. Cms 1763 dynamic list information. The completion of this form is needed to document your voluntary request for termination of medicare coverage as permitted under the code of federal regulations. Back to cms forms list; When do you use this application?
Cms 1763 Fillable, Printable PDF Template
You can cancel part a only if you pay a premium for it. Request for termination of premium hospital insurance of supplementary medical insurance. The following provides access and/or information for many cms forms. • if you have premium part a or part b, but wish to no longer be enrolled. You may also use the search feature to more.

CMS 1763 How to opt out of your medicare insurance
• if you have premium part a or part b, but wish to no longer be enrolled. People with medicare premium part a or b who would like to terminate their hospital or medical insurance coverage. You may also use the search feature to more quickly locate information for a specific form. When do you use this application? Cms 1763.

Cms L564 Printable Form
Cms 1763 dynamic list information. • if you have premium part a or part b, but wish to no longer be enrolled. When do you use this application? The completion of this form is needed to document your voluntary request for termination of medicare coverage as permitted under the code of federal regulations. You may also use the search feature.
Form CMS1490S Fill Out, Sign Online and Download Fillable PDF
People with medicare premium part a or b who would like to terminate their hospital or medical insurance coverage. The following provides access and/or information for many cms forms. Cms 1763 dynamic list information. When do you use this application? The completion of this form is needed to document your voluntary request for termination of medicare coverage as permitted under.
Fillable Request For Termination Of Premium Hospital And/or
You may also use the search feature to more quickly locate information for a specific form. Cms 1763 dynamic list information. Request for termination of premium hospital insurance of supplementary medical insurance. People with medicare premium part a or b who would like to terminate their hospital or medical insurance coverage. You can cancel part a only if you pay.
Back To Cms Forms List;
Request for termination of premium hospital insurance of supplementary medical insurance. The completion of this form is needed to document your voluntary request for termination of medicare coverage as permitted under the code of federal regulations. • if you have premium part a or part b, but wish to no longer be enrolled. You can cancel part a only if you pay a premium for it.
Cms 1763 Dynamic List Information.
The following provides access and/or information for many cms forms. You may also use the search feature to more quickly locate information for a specific form. When do you use this application? People with medicare premium part a or b who would like to terminate their hospital or medical insurance coverage.