Dental Clearance Form For Orthodontic Treatment
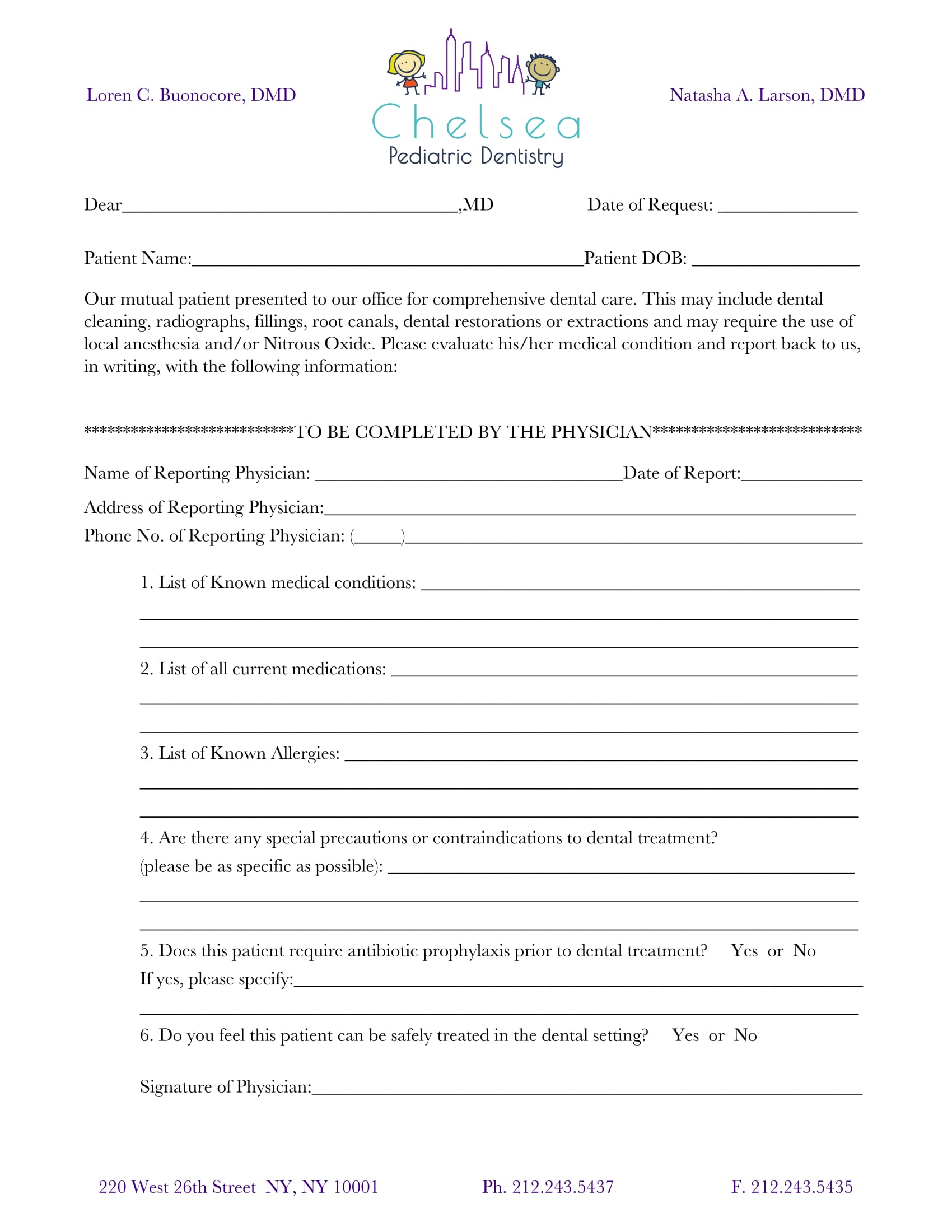
Dental Clearance Form For Orthodontic Treatment - Please also provide a restorative and periodontal clearance to begin orthodontic treatment. We look forward to working with you. Please provide us with the. _____the patient has all needed dental treatment completed and is able to start orthodontic treatment. *please have this form filled out by your dentist or dental hygienist. Prior to surgery, it is important to verify that the patient has had a dental exam within the past 6 months, has no current dental infection, no active. Please complete the following for our mutual patient who has scheduled an orthodontic appointment in our office. In order to start treatment, we require clearance from their general. We require that all of our patients are up to date with their general dental care before we can initiate orthodontic treatment. The patient noted above is interested in starting orthodontic treatment at our office.
Please also provide a restorative and periodontal clearance to begin orthodontic treatment. *please have this form filled out by your dentist or dental hygienist. Prior to surgery, it is important to verify that the patient has had a dental exam within the past 6 months, has no current dental infection, no active. We look forward to working with you. In order to start treatment, we require clearance from their general. _____the patient has all needed dental treatment completed and is able to start orthodontic treatment. Please provide us with the. We require this form to be completed before orthodontic treatment. The patient noted above is interested in starting orthodontic treatment at our office. We require that all of our patients are up to date with their general dental care before we can initiate orthodontic treatment.
Please provide us with the. *please have this form filled out by your dentist or dental hygienist. We require that all of our patients are up to date with their general dental care before we can initiate orthodontic treatment. _____the patient has all needed dental treatment completed and is able to start orthodontic treatment. In order to start treatment, we require clearance from their general. The patient noted above is interested in starting orthodontic treatment at our office. Please complete the following for our mutual patient who has scheduled an orthodontic appointment in our office. Please also provide a restorative and periodontal clearance to begin orthodontic treatment. Prior to surgery, it is important to verify that the patient has had a dental exam within the past 6 months, has no current dental infection, no active. We look forward to working with you.
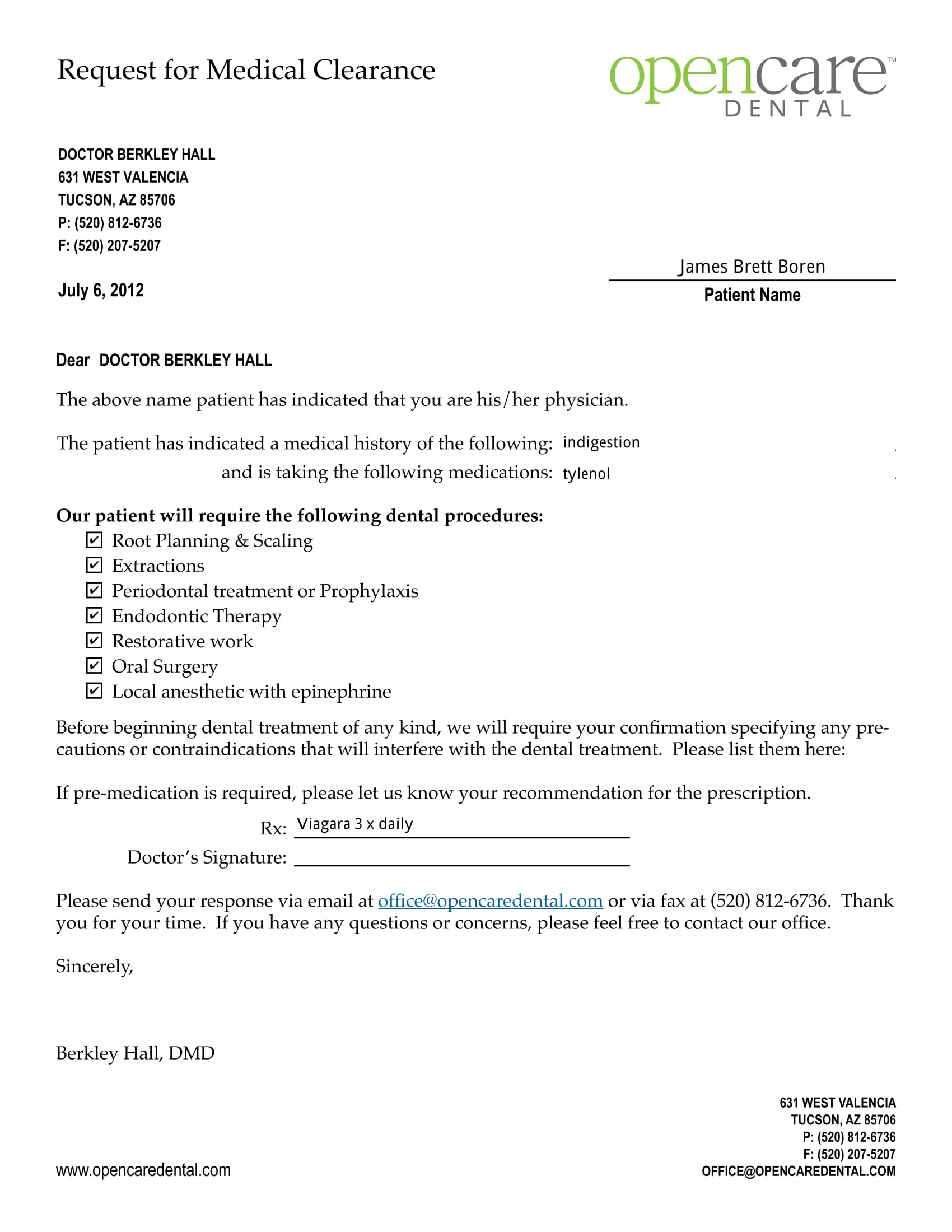
Printable Medical Clearance Form For Dental Treatment Printable Word
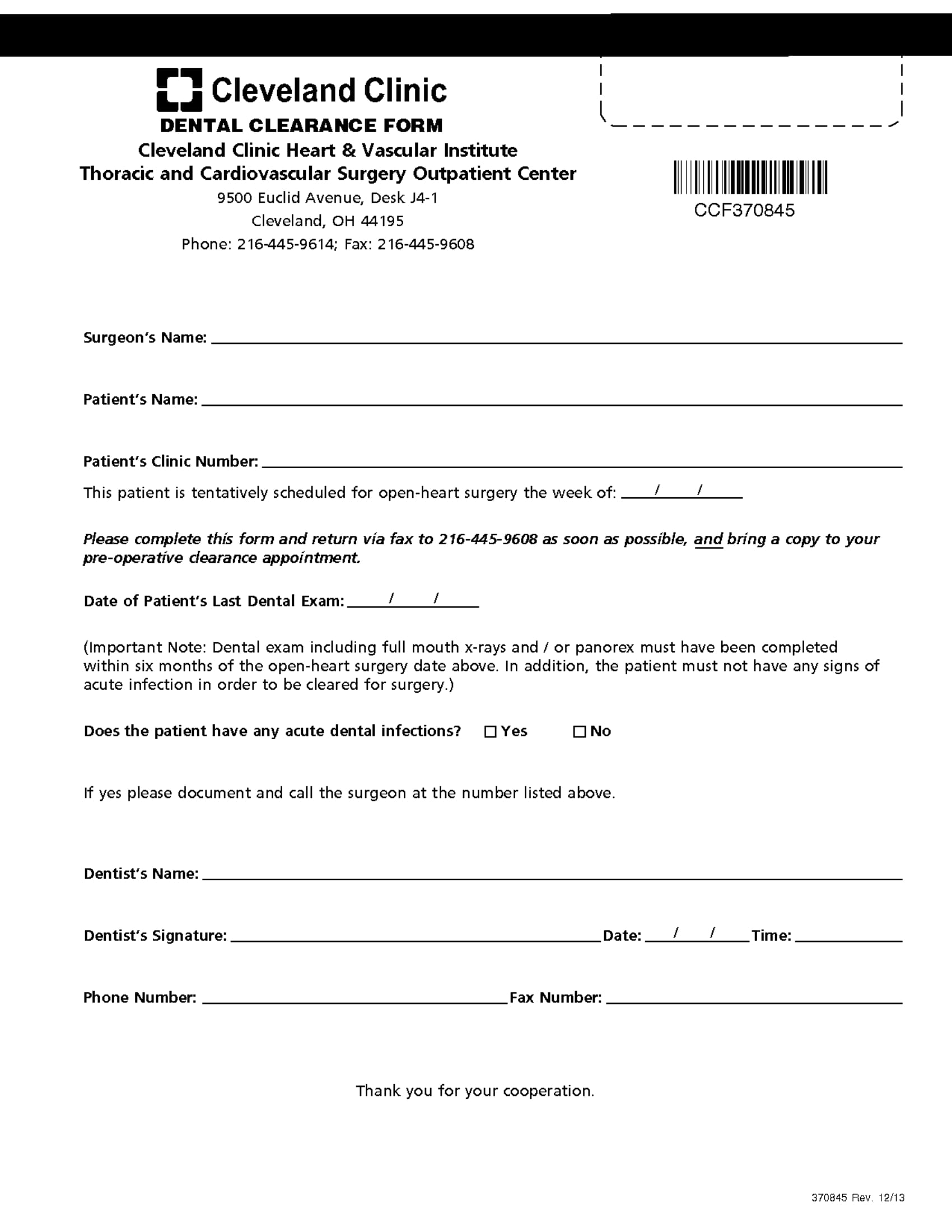
_____the patient has all needed dental treatment completed and is able to start orthodontic treatment. We require this form to be completed before orthodontic treatment. Prior to surgery, it is important to verify that the patient has had a dental exam within the past 6 months, has no current dental infection, no active. *please have this form filled out by.
FREE 18+ Dental Medical Clearance Form Samples, PDF, MS Word, Google Docs
The patient noted above is interested in starting orthodontic treatment at our office. Please provide us with the. _____the patient has all needed dental treatment completed and is able to start orthodontic treatment. We require this form to be completed before orthodontic treatment. Please complete the following for our mutual patient who has scheduled an orthodontic appointment in our office.
Printable Dental Clearance Form Printable Forms Free Online
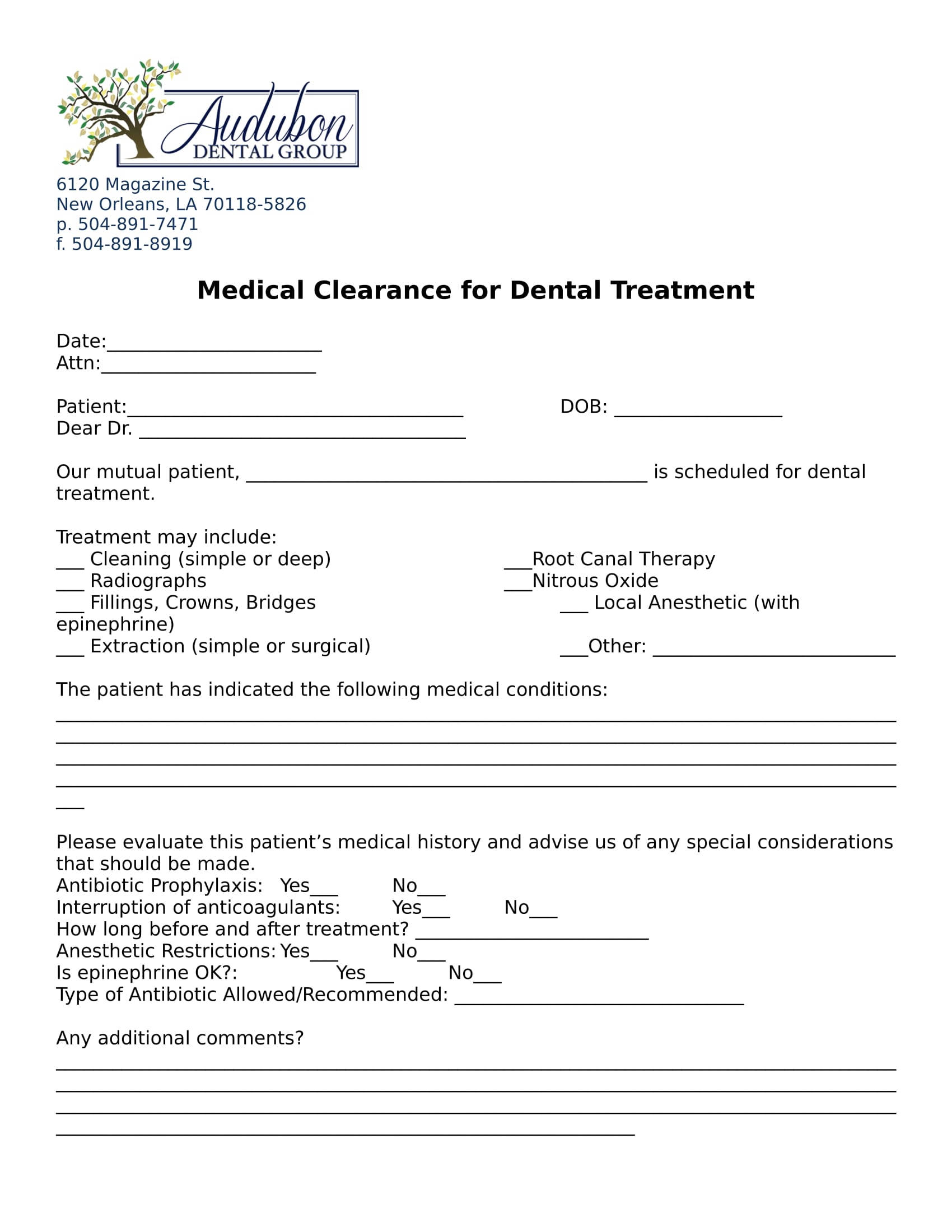
We require that all of our patients are up to date with their general dental care before we can initiate orthodontic treatment. We look forward to working with you. _____the patient has all needed dental treatment completed and is able to start orthodontic treatment. Please also provide a restorative and periodontal clearance to begin orthodontic treatment. *please have this form.
FREE 18+ Dental Medical Clearance Form Samples, PDF, MS Word, Google Docs
Prior to surgery, it is important to verify that the patient has had a dental exam within the past 6 months, has no current dental infection, no active. We look forward to working with you. In order to start treatment, we require clearance from their general. *please have this form filled out by your dentist or dental hygienist. Please also.
FREE 18+ Dental Medical Clearance Form Samples, PDF, MS Word, Google Docs
Please also provide a restorative and periodontal clearance to begin orthodontic treatment. Please complete the following for our mutual patient who has scheduled an orthodontic appointment in our office. We require this form to be completed before orthodontic treatment. The patient noted above is interested in starting orthodontic treatment at our office. *please have this form filled out by your.
FREE 18+ Dental Medical Clearance Form Samples, PDF, MS Word, Google Docs
In order to start treatment, we require clearance from their general. Please also provide a restorative and periodontal clearance to begin orthodontic treatment. We look forward to working with you. The patient noted above is interested in starting orthodontic treatment at our office. Please complete the following for our mutual patient who has scheduled an orthodontic appointment in our office.
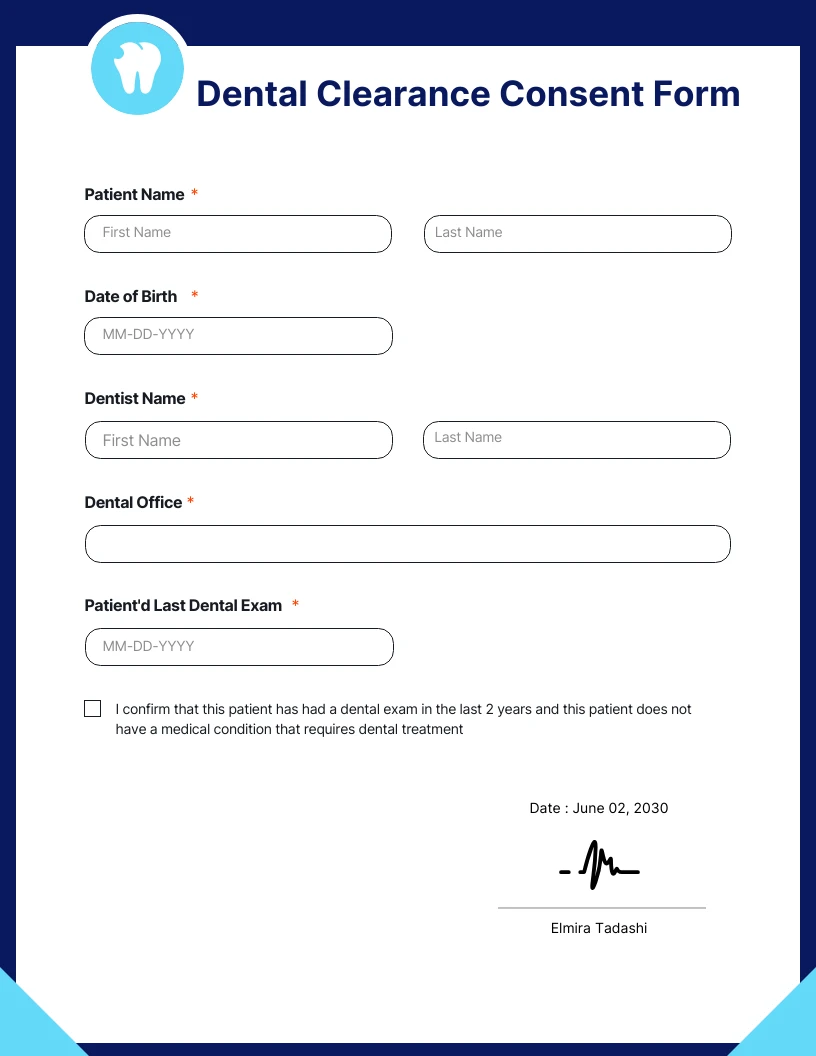
Dental Clearance Consent Form Template Venngage
Please provide us with the. Please complete the following for our mutual patient who has scheduled an orthodontic appointment in our office. We require that all of our patients are up to date with their general dental care before we can initiate orthodontic treatment. _____the patient has all needed dental treatment completed and is able to start orthodontic treatment. We.
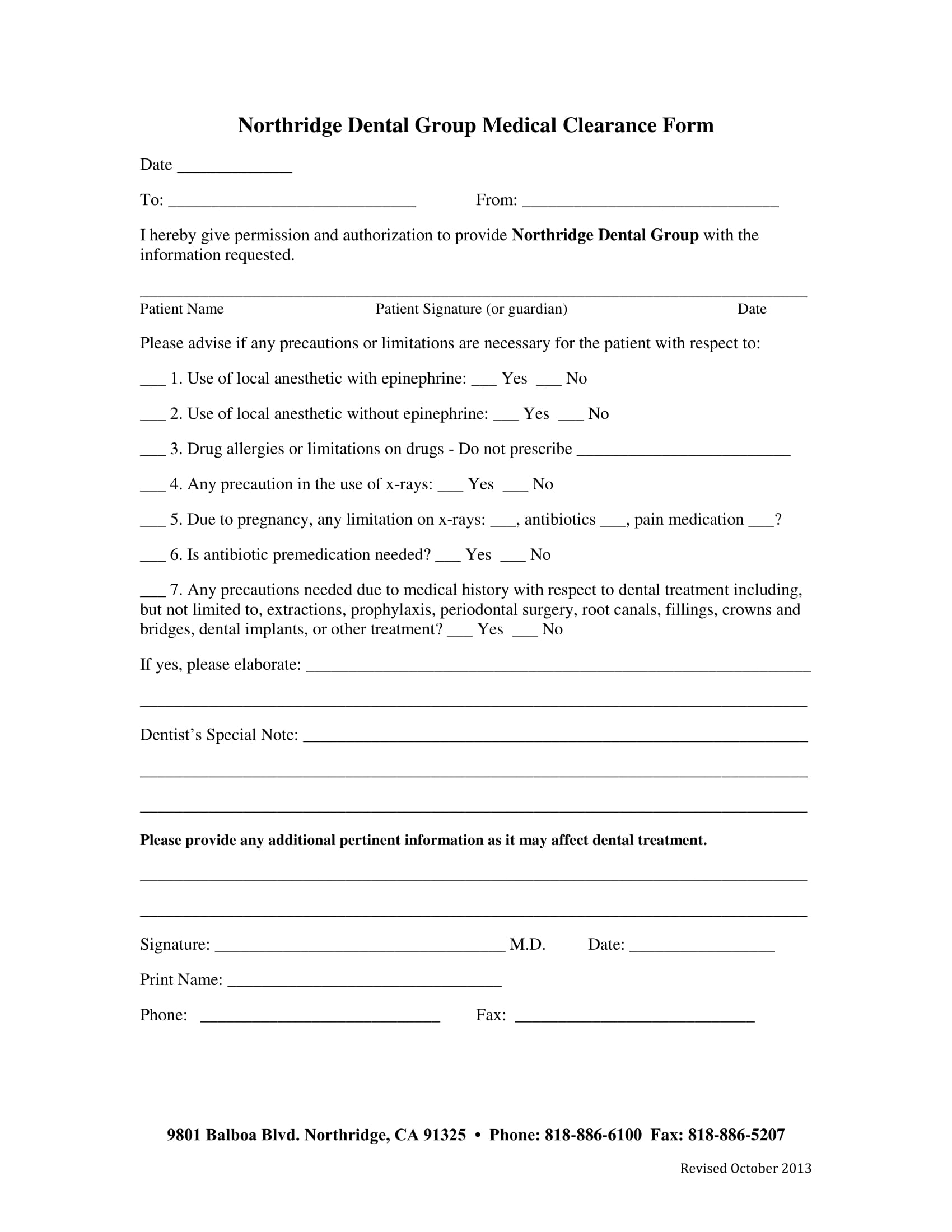
Printable Medical Clearance Form For Dental Printable Forms Free Online
In order to start treatment, we require clearance from their general. Please complete the following for our mutual patient who has scheduled an orthodontic appointment in our office. _____the patient has all needed dental treatment completed and is able to start orthodontic treatment. We require that all of our patients are up to date with their general dental care before.
Printable Medical Clearance Form For Dental Treatment Printable Word
We look forward to working with you. The patient noted above is interested in starting orthodontic treatment at our office. *please have this form filled out by your dentist or dental hygienist. Please complete the following for our mutual patient who has scheduled an orthodontic appointment in our office. Prior to surgery, it is important to verify that the patient.
FREE 18+ Dental Medical Clearance Form Samples, PDF, MS Word, Google Docs
Please complete the following for our mutual patient who has scheduled an orthodontic appointment in our office. We require that all of our patients are up to date with their general dental care before we can initiate orthodontic treatment. Please also provide a restorative and periodontal clearance to begin orthodontic treatment. Prior to surgery, it is important to verify that.
We Look Forward To Working With You.
The patient noted above is interested in starting orthodontic treatment at our office. Please complete the following for our mutual patient who has scheduled an orthodontic appointment in our office. We require that all of our patients are up to date with their general dental care before we can initiate orthodontic treatment. We require this form to be completed before orthodontic treatment.
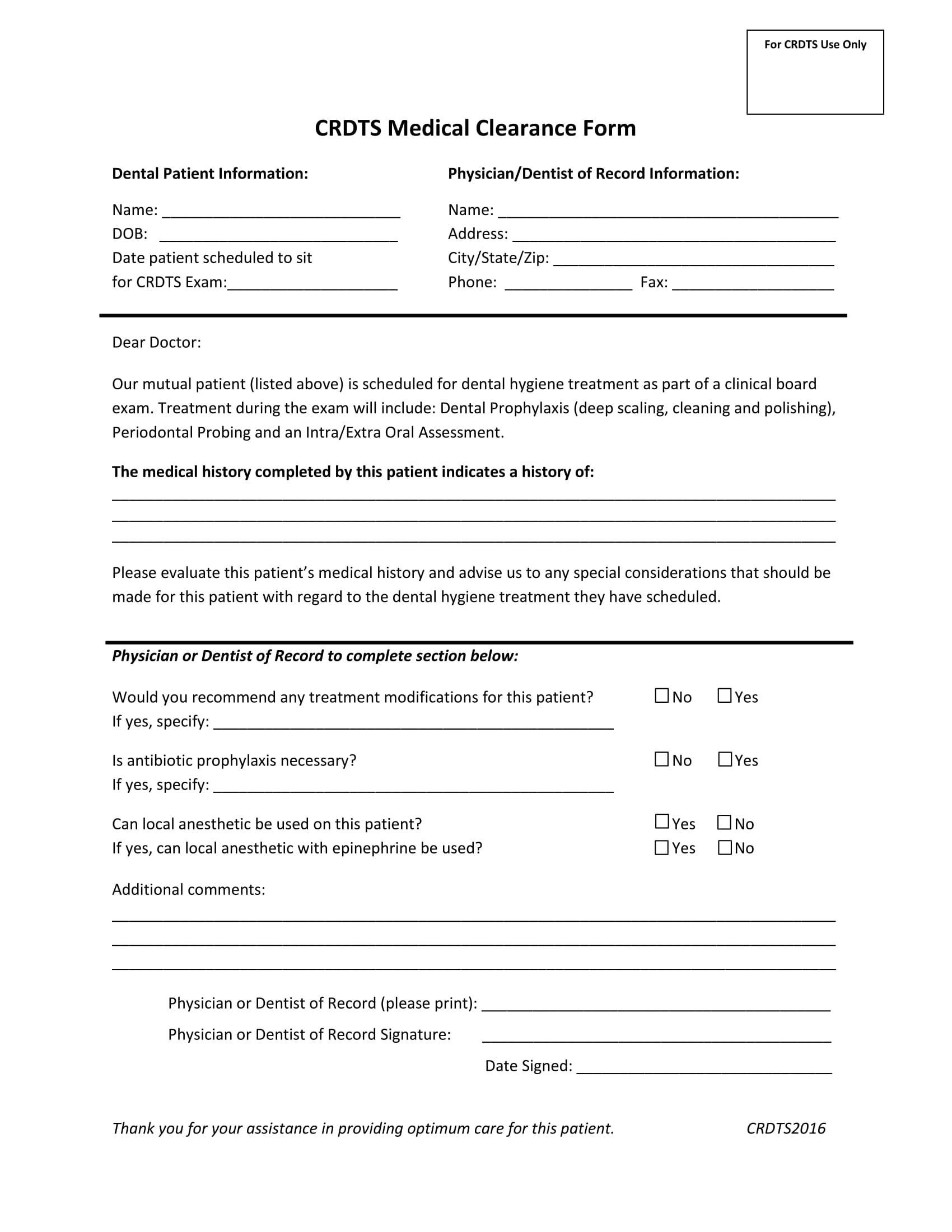
Prior To Surgery, It Is Important To Verify That The Patient Has Had A Dental Exam Within The Past 6 Months, Has No Current Dental Infection, No Active.
Please also provide a restorative and periodontal clearance to begin orthodontic treatment. *please have this form filled out by your dentist or dental hygienist. _____the patient has all needed dental treatment completed and is able to start orthodontic treatment. Please provide us with the.