Hipaa Release Form For 18 Year Old
Hipaa Release Form For 18 Year Old - 18 and older hipaa release and consent patient authorization for use and disclosure of protected health information (complete. Over 18 hipaa release and consent form except as i otherwise authorized below, as of my 18th birthday, my parents and/or guardians will no. I understand and acknowledge that as of my eighteenth (18) my parents and / or guardians birthday will no longer be permitted access to. I understand and acknowledge that as of my 18th birthday, my parents and / or guardians will no longer be permitted access to my medical.
Over 18 hipaa release and consent form except as i otherwise authorized below, as of my 18th birthday, my parents and/or guardians will no. 18 and older hipaa release and consent patient authorization for use and disclosure of protected health information (complete. I understand and acknowledge that as of my eighteenth (18) my parents and / or guardians birthday will no longer be permitted access to. I understand and acknowledge that as of my 18th birthday, my parents and / or guardians will no longer be permitted access to my medical.
I understand and acknowledge that as of my 18th birthday, my parents and / or guardians will no longer be permitted access to my medical. I understand and acknowledge that as of my eighteenth (18) my parents and / or guardians birthday will no longer be permitted access to. Over 18 hipaa release and consent form except as i otherwise authorized below, as of my 18th birthday, my parents and/or guardians will no. 18 and older hipaa release and consent patient authorization for use and disclosure of protected health information (complete.

HIPAA Release Template
18 and older hipaa release and consent patient authorization for use and disclosure of protected health information (complete. I understand and acknowledge that as of my eighteenth (18) my parents and / or guardians birthday will no longer be permitted access to. I understand and acknowledge that as of my 18th birthday, my parents and / or guardians will no.

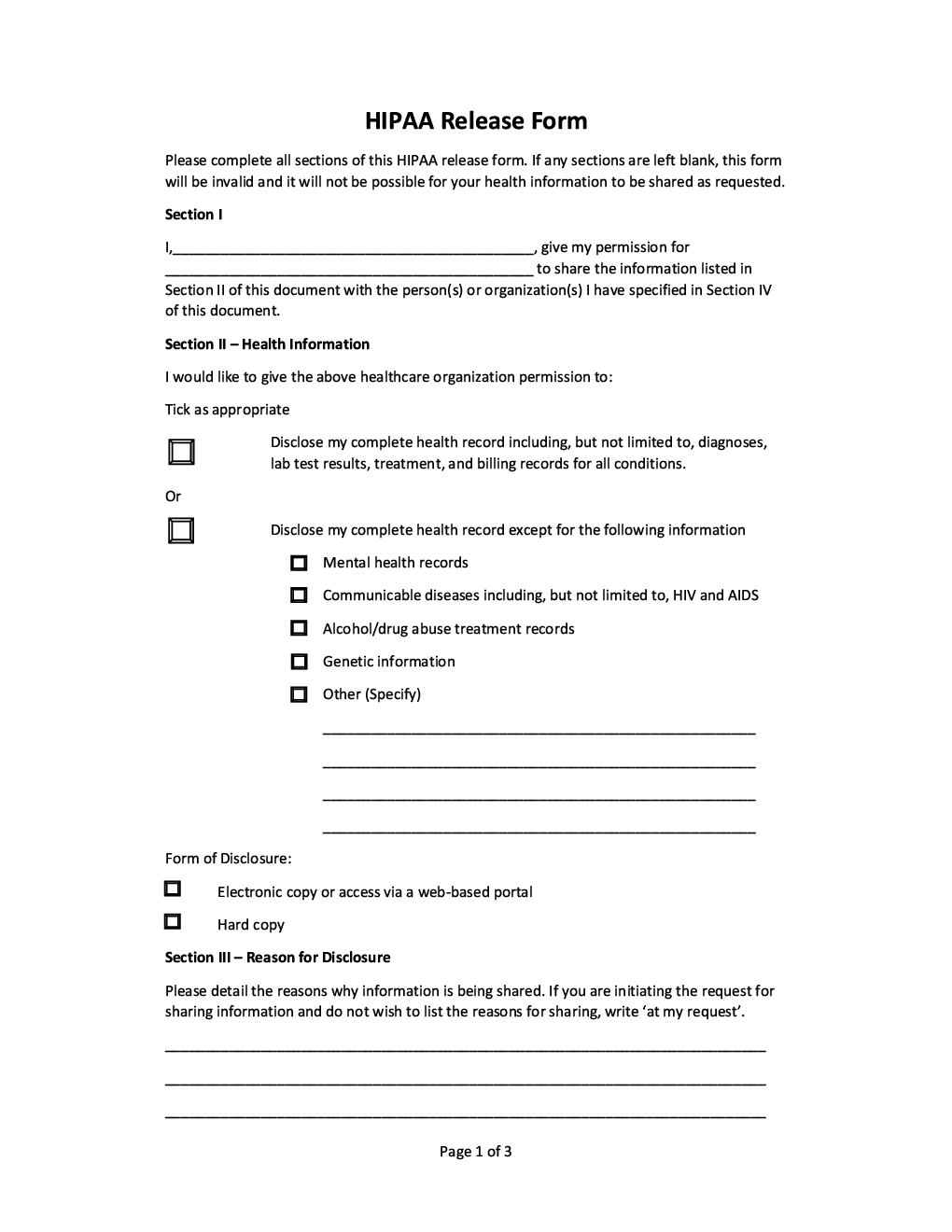
Developing Medical Authorization Forms HIPAA Release Form Guide
I understand and acknowledge that as of my eighteenth (18) my parents and / or guardians birthday will no longer be permitted access to. Over 18 hipaa release and consent form except as i otherwise authorized below, as of my 18th birthday, my parents and/or guardians will no. I understand and acknowledge that as of my 18th birthday, my parents.

Free Consent Forms (22) Sample Word PDF eForms
18 and older hipaa release and consent patient authorization for use and disclosure of protected health information (complete. I understand and acknowledge that as of my eighteenth (18) my parents and / or guardians birthday will no longer be permitted access to. Over 18 hipaa release and consent form except as i otherwise authorized below, as of my 18th birthday,.
Printable Hipaa Release Form
Over 18 hipaa release and consent form except as i otherwise authorized below, as of my 18th birthday, my parents and/or guardians will no. I understand and acknowledge that as of my 18th birthday, my parents and / or guardians will no longer be permitted access to my medical. 18 and older hipaa release and consent patient authorization for use.
HIPAA release form Forms Docs 2023
I understand and acknowledge that as of my 18th birthday, my parents and / or guardians will no longer be permitted access to my medical. 18 and older hipaa release and consent patient authorization for use and disclosure of protected health information (complete. I understand and acknowledge that as of my eighteenth (18) my parents and / or guardians birthday.
Hipaa Privacy Printable Hipaa Form Printable Forms Free Online
I understand and acknowledge that as of my 18th birthday, my parents and / or guardians will no longer be permitted access to my medical. Over 18 hipaa release and consent form except as i otherwise authorized below, as of my 18th birthday, my parents and/or guardians will no. 18 and older hipaa release and consent patient authorization for use.

Free Medical Records Release Form (HIPAA) PDF Word
18 and older hipaa release and consent patient authorization for use and disclosure of protected health information (complete. Over 18 hipaa release and consent form except as i otherwise authorized below, as of my 18th birthday, my parents and/or guardians will no. I understand and acknowledge that as of my 18th birthday, my parents and / or guardians will no.
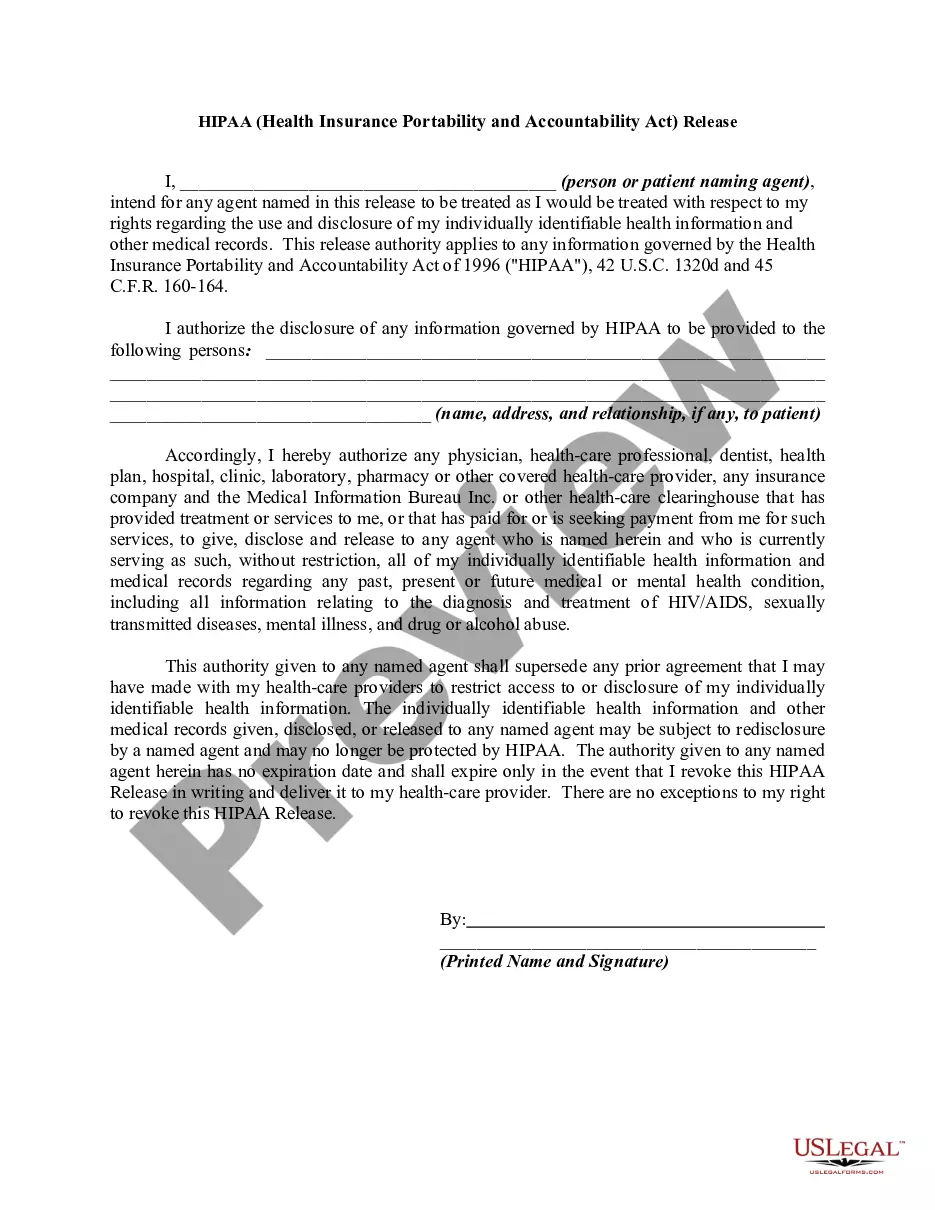
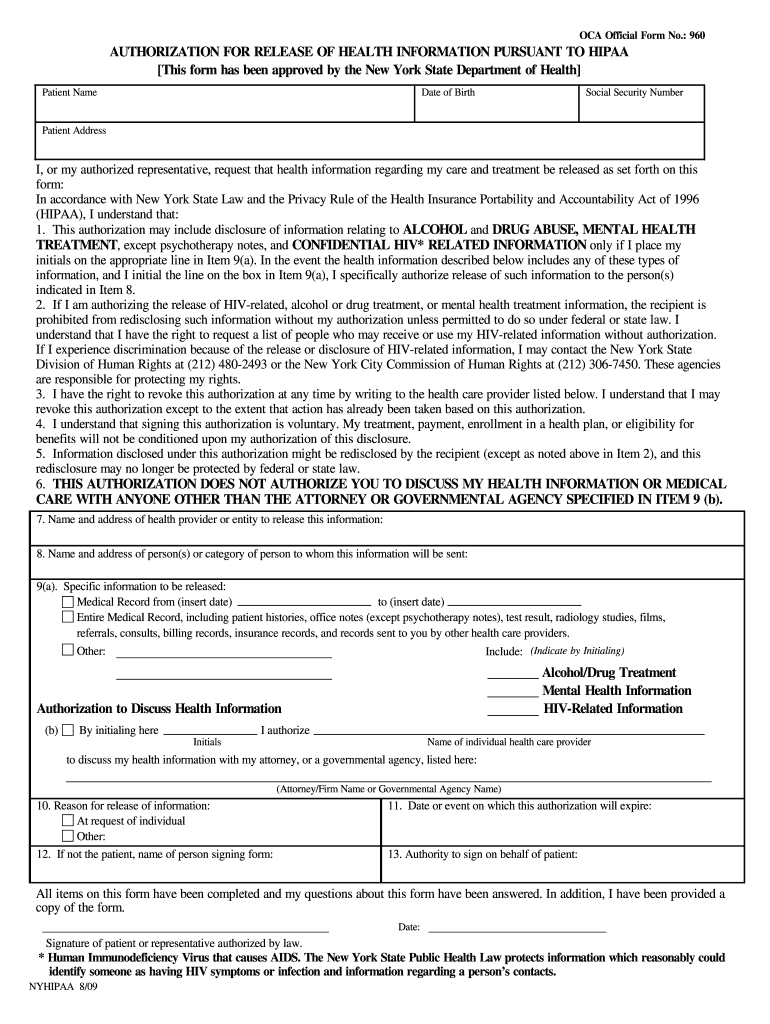
Hipaa Release Form For 18 Yearold US Legal Forms
I understand and acknowledge that as of my eighteenth (18) my parents and / or guardians birthday will no longer be permitted access to. I understand and acknowledge that as of my 18th birthday, my parents and / or guardians will no longer be permitted access to my medical. 18 and older hipaa release and consent patient authorization for use.
Medical Records Release Authorization Form For Free
I understand and acknowledge that as of my 18th birthday, my parents and / or guardians will no longer be permitted access to my medical. Over 18 hipaa release and consent form except as i otherwise authorized below, as of my 18th birthday, my parents and/or guardians will no. I understand and acknowledge that as of my eighteenth (18) my.
Patient Free Printable Hipaa Forms
I understand and acknowledge that as of my eighteenth (18) my parents and / or guardians birthday will no longer be permitted access to. I understand and acknowledge that as of my 18th birthday, my parents and / or guardians will no longer be permitted access to my medical. Over 18 hipaa release and consent form except as i otherwise.
18 And Older Hipaa Release And Consent Patient Authorization For Use And Disclosure Of Protected Health Information (Complete.
I understand and acknowledge that as of my eighteenth (18) my parents and / or guardians birthday will no longer be permitted access to. Over 18 hipaa release and consent form except as i otherwise authorized below, as of my 18th birthday, my parents and/or guardians will no. I understand and acknowledge that as of my 18th birthday, my parents and / or guardians will no longer be permitted access to my medical.